Percentage of motile spermatozoa at 22 hours after swim-up procedure: An indicator for intracytoplasmic sperm injection?
Article information
Abstract
Objective
The decision to use in vitro fertilization (IVF), intracytoplasmic sperm injection (ICSI), or split insemination (IVF-ICSI) in the first cycle is based on the number of motile sperm. Hence, total fertilization failure (TFF) often occurs during IVF cycles, despite normozoospermia. To investigate whether the cumulative motile swim-up spermatozoa percentage at 22 hours post-insemination (MSPPI) is an indicator for ICSI, we analyzed TFF, fertilization, blastocyst development, chemical pregnancy, clinical pregnancy, and live birth rates.
Methods
This prospective study was performed using data obtained from 260 IVF cycles. At 22 hours after insemination, the remaining swim-up spermatozoa were observed and divided into six groups according to MSPPI (<10%, 10% to <30%, 30% to <50%, 50% to <70%, 70% to <90%, and 90% to 100%).
Results
Regardless of the ejaculated motile sperm concentration (0.6–280×106/mL motile spermatozoa), the incidence of TFF significantly increased when MSPPI was <10%, and the fertilization rate significantly decreased when MSPPI was <30%. We found that cumulative MSPPI correlated with the cumulative fertilization rate (Spearman correlation, 0.508, p<0.001). Regarding embryo development, we observed no significant differences in the rates of blastocyst development, chemical pregnancy, clinical pregnancy, or live birth among all groups.
Conclusion
Our findings suggest that MSPPI is a viable indicator for split IVF-ICSI and ICSI. Taken together, by employing the MSPPI test in advance before IVF, ICSI, or split IVF-ICSI cycles, unnecessary split IVF-ICSI and ICSI may be avoided.
Introduction
Total fertilization failure (TFF) occurs in 5%-25% of conventional in vitro fertilization (IVF) cycles [123]. The main causes of TFF and low fertilization rate, defined as a fertilization rate of <25% during IVF, are defective sperm-zona pellucida binding or sperm penetration, which are mainly due to abnormalities in the sperm and not in the oocytes themselves [4].
To avoid a complete failure of IVF, rescue intracytoplasmic sperm injection (ICSI) [56,7,8] and split insemination (IVF-ICSI) [9] are often performed. The decision to use IVF, ICSI, or split IVF-ICSI is based on the number of motile sperm evident in the first cycle. A European Society of Human Reproduction and Embryology position paper [10] suggested that ICSI should be considered in cases of severe sperm abnormalities or in patients with a history of fertilization failure with conventional IVF attempts. However, ICSI is not the most suitable treatment for pathologies in women, such as poor ovarian response or previous implantation failures. This is consistent with the opinions of the Practice Committees of the American Society for Reproductive Medicine and Society for Assisted Reproductive Technology [11], and the Japan Society of Obstetrics and Gynecology [12]. Therefore, unnecessary ICSI should be avoided. However, because these committees do not provide concrete criteria (e.g., numbers of motile sperm) regarding the indications for ICSI, each hospital/clinic follows its own ICSI criteria. Our ICSI criteria comprise the following: (1) after sperm preparation, when no progressive motile spermatozoa are observed (e.g., spermatozoa in which only a flagellar beat can be observed); (2) after sperm preparation, when insufficient numbers of progressive motile spermatozoa are obtained (<20,000 spermatozoa/oocyte); (3) IVF has failed completely twice in a row (in case of TFF, at first cycle, IVF is performed, at second cycle, split IVF–ICSI is performed, and at third cycle, ICSI is performed); or (4) patients strongly request ICSI.
Rescue ICSI complies with the need to avoid unnecessary ICSI. Previous studies have reported that rescue ICSI is performed at 22 hours [5], 6 hours [7], or 3 hours [8] post-insemination. The fertilization and implantation rates of rescue ICSI were significantly lower after 22 hours than after 6 hours because of oocyte aging [7]. A cost-effectiveness analysis of rescue ICSI showed a 25% reduction in the cost per live birth, even when rescue ICSI was performed at 1 day after insemination, compared with cycle cancelation [13]. Accordingly, early rescue ICSI, performed as early as 6 hours after insemination, is an effective backup treatment to avoid TFF [6]. However, the rate of polyspermy was significantly higher with early rescue ICSI than with ICSI [14]. Moreover, Vitek et al. [15] demonstrated that IVF is preferable because of its increased live birth rate relative to split IVF-ICSI and ICSI in a single cycle. Therefore, to avoid unnecessary ICSI, a predictor of fertilization is crucial.
Coccia et al. [16] reported that a sperm survival test (SST) may predict the outcome of IVF in the presence of male factor infertility. In contrast, several studies have asserted that the percentage of sperm motility at 24 hours and the sperm survival ratio in both semen and sperm suspension for insemination have no practical value in predicting fertilization in vitro [1718]. Eskandar [18] reported that the fertilization rate decreases when the percentage of motile spermatozoa is 0% at 24 hours after insemination. In our study, we focused on the relationship between the motile swim-up spermatozoa percentage at 22 hours post-insemination (MSPPI, our calculation method differed from that of the SST) and on the fertilization rate, because we have rarely observed motile sperm during 1 day-old rescue ICSI at 22 hours after insemination in patients with TFF and low fertilization rate (unpublished data). The relationship between SST and the fertilization rate has been investigated, but few studies have discussed single sperm analysis and the impact on embryo development/pregnancy rates. In this study, we investigated the relationship between the cumulative MSPPI and fertilization/embryo development/pregnancy rates.
Methods
1. Patients
This prospective study was performed using data obtained from 260 IVF cycles performed between July 2013 and July 2014 and frozen blastocyst transfer (FBT) cycles derived from these IVF cycles. Informed consent was obtained for all procedures. All procedures were performed in accordance with the Declaration of Helsinki.
2. Ovarian stimulation
Ovarian stimulation was performed as previously described [19]. Briefly, long, short, or gonadotropin-releasing hormone (GnRH)-antagonist protocols were used depending on the patient. In poor responders who have ≤2 follicles even if they were injected with human menopausal gonadotropin (hMG; ASKA Pharmaceutical Co., Tokyo, Japan) several times before during previous infertility treatment, including timing treatment or artificial insemination with sperm from the patient's husband, in combination with herbal medicine, clomifene citrate (50 mg Spacromin tablet, Pola Pharma Inc., Tokyo, Japan) and hMG were used for ovarian stimulation [20]. A GnRH analogue acetate (Fuji Pharma Co., Tokyo, Japan), hMG, and a GnRH antagonist (Cetrotide, Shionogi & Co., Osaka, Japan) were used in each protocol. When at least two follicles reached 18 to 20 mm in diameter (as determined by transvaginal ultrasonography), 5,000 IU of human chorionic gonadotropin (Fuji Pharma Co.) was administered. Ovum pickup was performed 35 hours after the human chorionic gonadotropin injection.
3. Collection of sperm/IVF
Ejaculated sperm were collected and incubated for at least 1 hour. Semen samples were analyzed using a Makler Counting Chamber (Sefi Medical Instruments, Haifa, Israel). Semen samples were overlaid on to 90% ISolate (Irvine Scientific, Santa Ana, CA, USA) and then centrifuged at 1,000 revolutions per minute (rpm) for 10 minutes (Iuchi Centrifuge CN-10, AS ONE, Osaka, Japan). The upper layers were aspirated, and 1 mL of Universal IVF Medium (Origio, Måløv, Denmark) was added and pipetted with the pellet. The sperm sample was centrifuged at 1,000 rpm for 5 minutes. The supernatant was removed, and 0.5 to 1 mL of Universal IVF Medium was added to the pellet. Sperm samples were subjected to swim-up procedure for 10 minutes in an incubator. Swim-up spermatozoa were obtained. Approximately 10×104/mL swim-up sperm were added to a one-well IVF dish (Falcon, Corning Life Sciences, Tewksbury, MA, USA) containing <5 cumulus oocyte complexes in 1 mL of Universal IVF Medium. If no progressive motile spermatozoa were observed [21], ICSI was performed after the provision of informed consent. Fertilized eggs were cultured in continuous single culture medium (Irvine Scientific) with 10% serum substitute supplement (Irvine Scientific) until day 7 or when fresh embryo transfer was performed. The relationship between the ejaculated motile sperm concentration and fertilization rate during each IVF cycle was analyzed according to the split IVF-ICSI criteria set by Hashimoto et al. [22].
4. Swim-up spermatozoa analysis at 22 hours after insemination
At 22 hours after insemination, the remaining swim-up spermatozoa were examined at least twice per sample using a Makler Counting Chamber and divided into six groups according to their MSPPI (group A, <10%; group B, 10% to <30%; group C, 30% to <50%; group D, 50% to <70%; group E, 70% to <90%; and group F, 90% to 100%). MSPPI was calculated as the ratio between the motile spermatozoa (progressive motile and non-progressive motile spermatozoa) [21] and total spermatozoa (motile and immotile spermatozoa) [21] at 22 hours post-insemination. To prevent bias in human analysis of the retrieved samples and to ensure objectivity, the category of motile sperm included even spermatozoa in which only a flagellar beat could be observed, according to the World Health Organization Laboratory Manual for the Examination and Processing of Human Semen [21].
5. Cryopreservation/thawing/blastocyst transfer
Blastocysts were cryopreserved and thawed using the Cryotop technique, as previously described [23], with the modification that thawing was performed at room temperature. One frozen-thawed blastocyst was transferred to the uterus of each patient. Luteal support for FBT cycles was performed as previously described [24]. Briefly, patients received 2 mg of chlormadinone acetate (Lutoral, Shionogi & Co.) three times daily after ovulation, and 0.72 mg transdermal estradiol patches (Estrana Tape, Hisamitsu Pharmaceutical Co., Tokyo, Japan) were applied to the abdomen for 10 weeks after the initiation of menstruation. On the day of blastocyst transfer, if their serum progesterone concentration was <15 ng/mL, the women were injected with 125 mg of 17α-hydroxyprogesterone caproate once every 5 days. Moreover, patients took a 5 mg prednisolone tablet (Towa Pharmaceutical Co., Osaka, Japan) three times daily for 3 days after ovulation. The dosage of prednisolone was set at 15 mg/day based on a previous study [19]. Stimulation of the endometrium for embryo transfer [25] was performed 2 or 3 days before FBT.
6. Statistical analysis
Correlations between the fertilization rate and ejaculated motile sperm concentration and the fertilization rate and MSPPI were evaluated using the Spearman rank-order correlation coefficient (Spearman correlation, γs). The differences between the mean age of women, the mean number of oocytes recovered, and the number of motile spermatozoa in the original semen and after preparation were evaluated using one-factor analysis of variance. The mean age of the women was evaluated using the Tukey-Kramer post hoc test, and the mean number of oocytes recovered and number of motile spermatozoa were evaluated using the Steel-Dwass method. These data are presented as mean±standard deviation. The TFF, fertilization, blastocyst development, chemical pregnancy, clinical pregnancy, and live birth rates were evaluated using the chi-square test and residual analysis. A p-value of <0.05 was considered to indicate statistical significance.
Results
This study showed no correlation between the ejaculated motile sperm concentration (0.6–280×106/mL motile spermatozoa) and fertilization rate in 260 IVF cycles (γs=-0.079, P=0.357) (Figure 1). Moreover, we analyzed the relationship between the frequency of a <30% fertilization rate and sperm concentration or motile sperm percentage in original semen according to the criteria of Hashimoto et al. [22] (an original sperm concentration of <20×106/mL or original motile sperm percentage of <20%), which were based on a <30% fertilization rate. Our results did not meet these criteria (<20 vs. ≥20×106/mL sperm concentration in original semen, 5/29 cycles [17.2%] vs. 26/231 cycles [11.3%], p=0.348, respectively; and <20% vs. ≥20% motile sperm percentage in original semen, 2/6 cycles [33.3%] vs. 29/254 cycles [11.4%], p=0.102, respectively; data not shown).
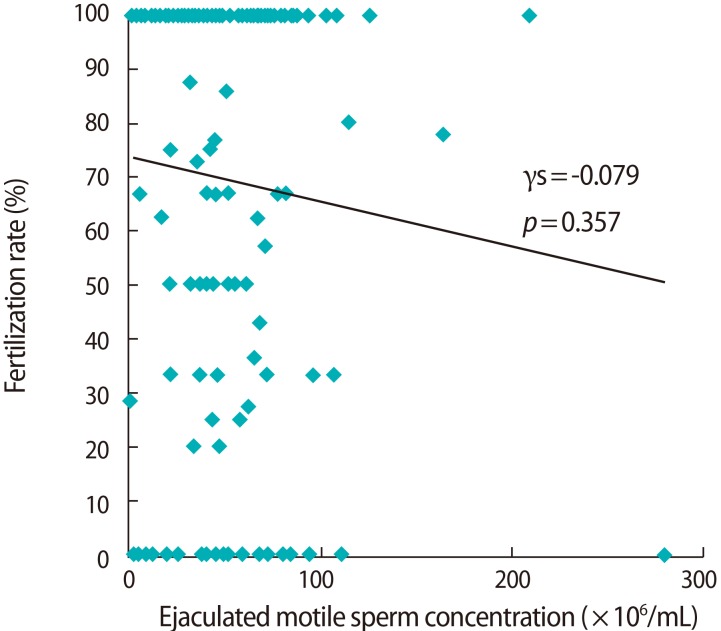
The correlation between ejaculated motile sperm concentration and fertilization rate during each in vitro fertilization cycle. The correlation was evaluated using the Spearman rank-order correlation coefficient (n=260 in vitro fertilization cycles).
Next, we investigated the relationship between the fertilization rate and MSPPI. No significant differences in patient backgrounds, except in the mean number of oocytes recovered (the mean age of the women and the number of motile spermatozoa in the original semen and after preparation were not significantly different), among the groups (Table 1). The mean number of oocytes recovered was significantly lower in group D than in groups E and F (Table 1). The incidence of TFF was significantly higher in group A than in the other groups (p=0.035). In groups A and B, the occurrence of two pronuclei and two polar bodies (2PN2PB) was significantly lower than in groups C to F (p=0.00007). Moreover, in groups A and B, the occurrence of unfertilized eggs was significantly higher than in the other groups (p<0.0001). Conversely, the incidence of TFF in group F was significantly lower than in the other groups (p=0.035) and the occurrence of 2PN2PB in group F was significantly higher than in the other groups (p=0.00007). Also, the occurrence of unfertilized eggs in groups E and F was significantly lower than in the other groups (p<0.001) (Table 2). Regarding embryo development, no significant differences were evident in the rates of blastocyst development, chemical pregnancy, clinical pregnancy, and live birth among the groups (Table 3).
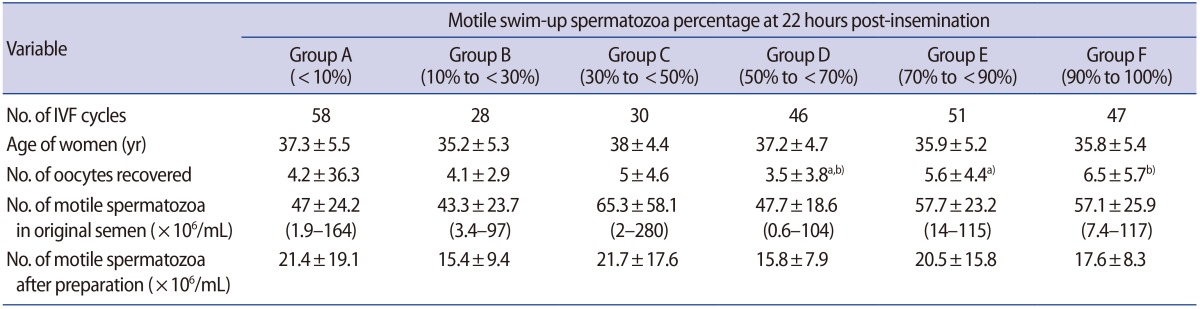
Patient backgrounds
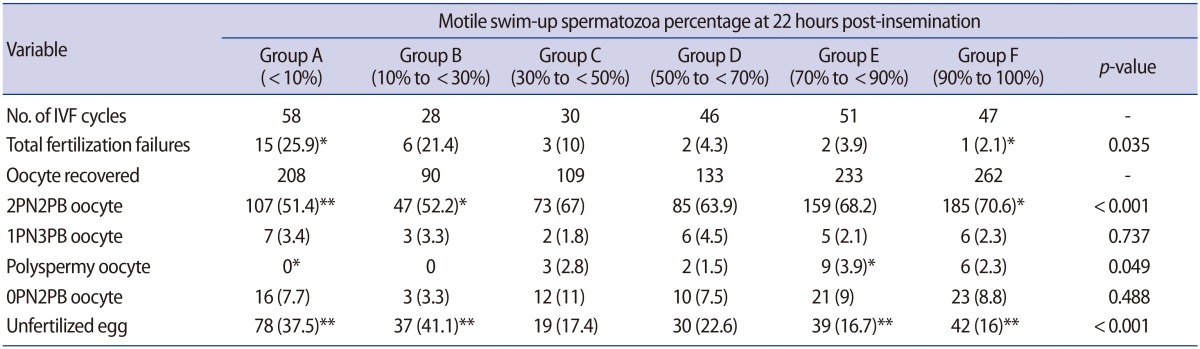
The relationship between fertilization rates and motile swim-up spermatozoa percentage at 22 hours post-insemination

Blastocyst development and embryo transfer outcome
We found a correlation between the cumulative MSPPI and cumulative fertilization rate in patients who underwent at least two cycles (γs=0.508, p<0.001) (Figure 2).
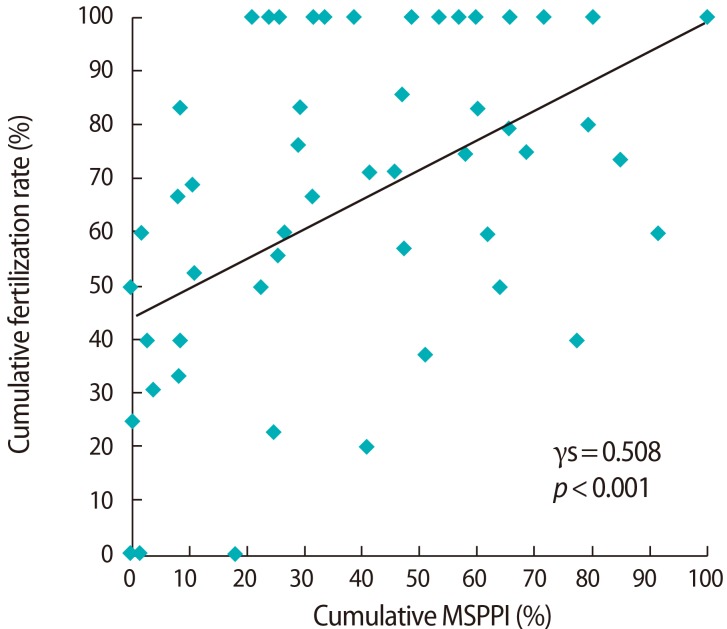
The correlation between cumulative motile swim-up spermatozoa percentage at 22 hours post-insemination and cumulative fertilization rate throughout all cycles in patients who received at least two in vitro fertilization cycles. The correlation was evaluated using the Spearman rank-order correlation coefficient (n=52 patients, 148 in vitro fertilization cycles).
Discussion
In this study, we showed that cumulative MSPPI is correlated with the cumulative fertilization rate. These results suggest that a low MSPPI value is a potential indicator for split IVF-ICSI and ICSI.
We began our study by investigating the correlation between the ejaculated motile sperm concentration and the fertilization rate during each IVF cycle. We showed that the fertilization rate was not correlated with the ejaculated motile sperm concentration. We evaluated our data using the criteria of Hashimoto et al. [22], and our findings were not consistent with theirs. This suggests that basing the decision to use IVF, ICSI, or split IVF-ICSI on the motile sperm concentration may lead to unnecessary ICSI.
In terms of predicting the fertility of cultured swim-up spermatozoa, our method was similar to SST; however, there were some differences in our calculation method. In particular, SST calculates the ratio between the final concentration of progressive spermatozoa after 24 hours and the initial concentration of progressive spermatozoa [17]. Our method, however, calculated the ratio between the motile sper-matozoa and total spermatozoa at 22 hours post-insemination.
Our results showed that, regardless of the ejaculated motile sperm concentration, the incidence of TFF significantly increases when MSPPI is <10% and that the fertilization rate significantly decreases when MSPPI is <30%. Tournaye et al. [2] reported that the incidence of TFF is higher when insemination is performed with 5,000 sperm/oocyte than when performed with 20,000 sperm/oocyte (25.7% vs. 5.3%). In this study, despite using an insemination concentration of >20,000 spermatozoa/oocyte, TFF occurred in 25.9% of patients when MSPPI was <10%. Accordingly, the main cause of TFF in this study is unlikely to be the number of motile spermatozoa/oocyte. Regarding embryo development, no significant differences were evident in the rates of blastocyst development, chemical pregnancy, clinical pregnancy, and live birth among the groups. These results suggest that MSPPI relates to the fertilization rate alone.
After sperm preparation techniques, such as swim-up procedure and density gradient centrifugation, intercellular reactive oxygen species (ROS) and hydrogen peroxide concentrations and DNA fragmentation in human spermatozoa increase [2627]. Tremellen [28] reported that ROS damage the sperm membrane, thus decreasing the motility of sperm and their ability to fuse with the oocyte. Also, ROS can alter sperm DNA, resulting in the passage of defective paternal DNA to the conceptus.
Moreover, ROS levels are higher in the semen of patients with astheno teratozoospermia and leukocytospermia than in those of normozoospermic individuals [29]. In a meta-analysis, Agarwal et al. [30] reported that fertilization rates after IVF correlate with seminal ROS levels. Our data showed a correlation between MSPPI and fertilization rate. We speculate that the resistance of spermatozoa to ROS may be an important factor in assisted reproductive technology.
There are some limitations in the present study. The first is that the analysis was based on cumulative data that were obtained from the relationship between fertilization and MSPPI in each patient as the main results. The data are obtained from two IVF cycles in cases of complete IVF failure, because we were investigating TFF patients who repeatedly failed to fertilize by IVF. An ICSI approach is a top priority method in the third cycle. A second limitation was that sperm analysis performed by embryologists may be less objective than computer-aided sperm analysis [3132]. However, to ensure objectivity, the category of motile sperm included even spermatozoa in which only a flagellar beat can be observed. Thus, we prevented bias in human analysis of sperm.
In conclusion, MSPPI may be a viable indicator for split IVF-ICSI and ICSI. By employing the MSPPI test during semen analysis and/or artificial insemination, unnecessary split IVF-ICSI and ICSI may be avoided.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.